
Peakspan: The True North of Longevity and Why We Must Aim Beyond Healthspan
Welcome to the Post-Healthspan Era: Peakspan is the Essential Metric for the Longevity Century

For over two decades, since I made the decision to leave a successful career in the IT industry to dedicate my life to longevity biotechnology, my singular, overarching goal has been to develop technologies that allow humans to age without losing their functional capacities—and to continuously improve. Throughout this journey, the scientific community has constantly debated the metrics by which we measure our success. How do we define quality of life? How do we quantify the exact biological milestones of aging? And most importantly, what exactly are we trying to optimize when we discover new interventions?
Today, I want to talk about a fundamental shift in how we must view human aging. We are entering the era of Pharmaceutical Superintelligence, an era where generative AI is discovering novel targets and designing completely new molecules in a fraction of the time it took just five years ago. Because our technological capabilities are accelerating at this unprecedented pace, our biological aspirations must accelerate with them.
We need a new metric. We need a concept that goes beyond simply keeping people out of the hospital. We need to introduce the world to Peakspan.

The Multidimensional and Multifactorial Reality of Aging
To understand why a new metric is necessary, we must first look at the harsh, multifactorial reality of human aging. Aging is not a monolithic, unified switch that flips in the human body. It is a highly complex, multidimensional, and multifactorial process.
If you look at human biology as an incredibly sophisticated piece of hardware - you realize that not all components wear out at the same time. Humans, in every physical and cognitive capability, age differently. Your immune system has its own clock. Your skeletal muscle has its own clock. Your reproductive system, your respiratory capacity, and your cognitive processing speed all operate on different, albeit interconnected, trajectories.
For every single biological system and capability, there is a distinct life cycle. First, there is a period of development leading to a peak. This is the apex of your functional capacity, the moment your biology operates at its absolute maximum efficiency. Following this peak, there is inevitably a trough—a plateau that slowly gives way to the next phase. Then begins the long, agonizing decline. During this decline, you might not be clinically “sick,” but you are losing capacity every single day. Your Forced Vital Capacity (FVC), the metric I care much about, drops every year after a certain age. Your VO2 max drops. Your reaction time slows. Your cellular repair mechanisms falter.
Eventually, this continuous decline crosses a clinical threshold, leading to multimorbidity—the simultaneous presence of two or more chronic medical conditions. This is the stage where the healthcare system finally intervenes, usually too late, attempting to manage symptoms rather than addressing the root cause. And finally, this multimorbidity culminates in death.
This is the cycle: Peak, Trough, Decline, Multimorbidity, and Death. For the entirety of human history, evolution has polished us to accept this paradigm. But evolution is a cruel master, and the inability to change this cycle is the ultimate restriction on human freedom and prosperity.
The Evolution of the Longevity Consensus: From Lifespan to Healthspan
In the early days of biogerontology, the primary metric of success was lifespan—the absolute number of years a biological organism survives. However, as the field matured, the public and policymakers began to express a very valid fear: what if we extend lifespan, but only extend the years of multimorbidity? No one wants to spend an extra two decades in a frail, disease-ridden state, reliant on continuous medical care.
In response to this, the longevity community made a brilliant, strategic, and necessary pivot. We rallied around the concept of healthspan. Healthspan is defined as the period of life spent free from chronic, debilitating disease.
I have profound respect for the pioneers who championed healthspan. It was exactly the conceptual shift we needed to legitimize aging research. It allowed us to align our goals with the broader medical community and government healthcare systems. Advocating for healthspan helped us shift the global conversation from “living longer” to “living healthier.” It was a critical stepping stone that brought credibility, funding, and brilliant minds into the longevity biotechnology ecosystem.
However, as science progresses, our metrics must evolve.
Recently, the longevity community has become incredibly comfortable—perhaps a bit too comfortable—with healthspan as the ultimate goal. The longevity community became too “woke” advocating for healthspan, transforming a necessary clinical endpoint into a psychological and philosophical ceiling. Very often I go to conferences and hear some of the prominent leaders saying “Oh no, we are not aiming to extend human lifespan, we only care about extending healthspan”. In reality, there is no intervention that can dramatically extend lifespan without significantly extending healthspan. While the intentions behind healthspan are pure and medically sound, relying on it as our final destination risks masking the silent, insidious erosion of human potential.
If we only measure the years free of diagnosable chronic disease, we inadvertently normalize the “healthy but declined” state. A 65-year-old who is free of cancer, Alzheimer’s, and heart disease is considered to be in their “healthspan.” But that same 65-year-old likely has significantly less muscle mass, lower energy levels, slower cognitive recall, and less physical endurance than they did at 25. They are healthy, yes, but their functional capacity is severely diminished.
By focusing solely on healthspan, we are setting the bar too low for the future of biotechnology. We are essentially saying that as long as you don’t have a recognizable disease, your biological state is acceptable. But the gradual erosion of your capabilities—the slow loss of your physical and mental vigor—is not acceptable. It restricts your freedom. It inhibits economic growth. We must not make an enemy of healthspan; rather, we must view it as the foundation upon which we build something far more ambitious.
Introducing Peakspan: The Ultimate Metric for Rejuvenation
This brings us to the new paradigm. In a recent perspective paper published in Aging and Disease, my colleagues Dominika Wilczok, Kejun Ying, and I introduced a new metric that redefines the goals of longevity biotechnology: Peakspan.
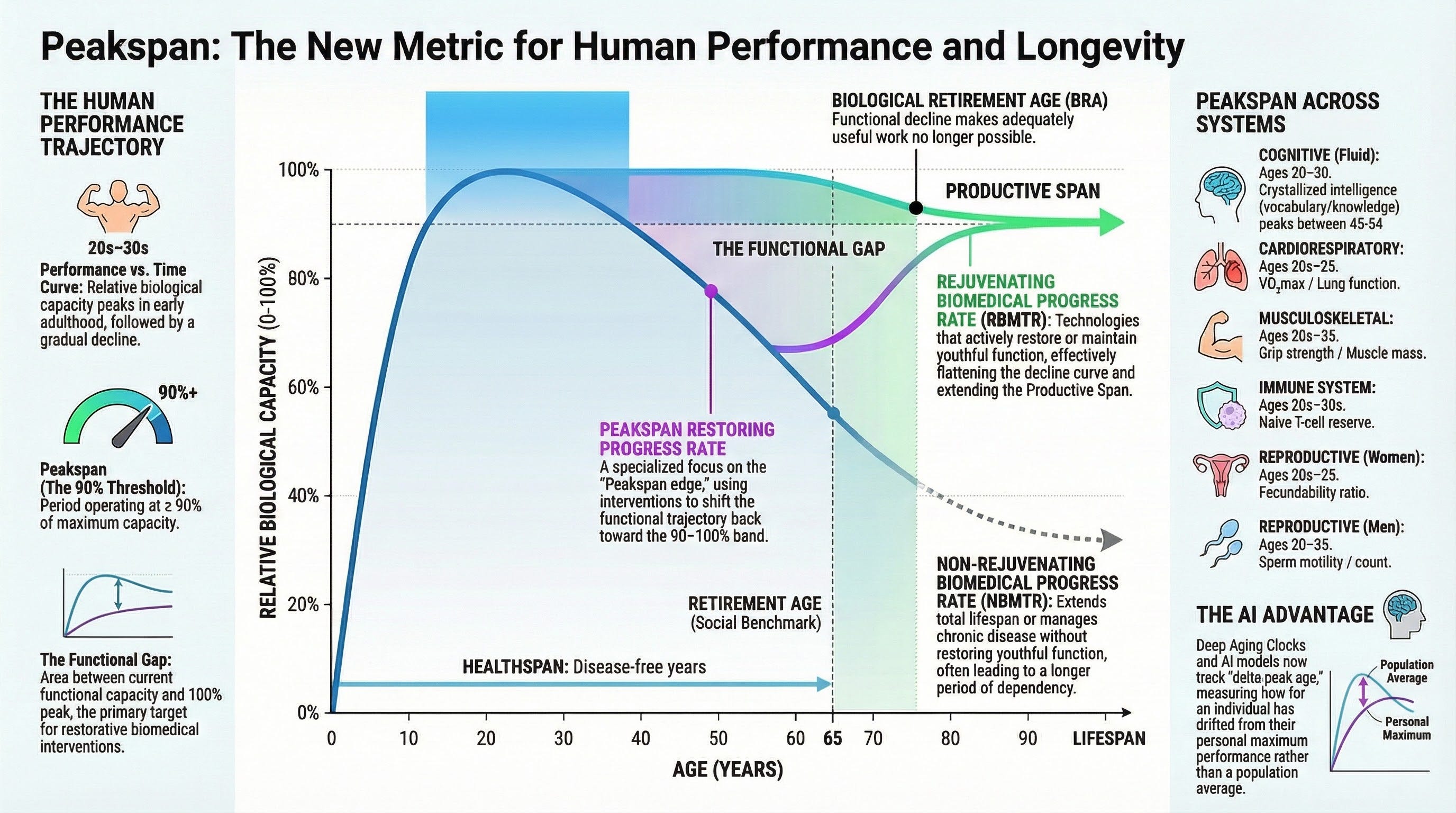
Peakspan is defined as the age interval during which an individual maintains at least 90% of their peak functional performance in a specific physiological or cognitive domain.
Unlike healthspan, which is a binary measure of “diseased” versus “not diseased,” Peakspan is a continuous, high-resolution metric of optimal functionality. When we conducted our multi-system analysis of human biology, we uncovered a profound and somewhat depressing misalignment: most human biological systems reach their maximal capacity in early adulthood, typically between the ages of 20 and 30.
This means that your Peakspan—the time you spend at or above 90% of your maximum biological capacity—is remarkably short relative to your total lifespan. A person might live to be 85, and they might remain free of chronic disease until they are 75 (their healthspan). But their Peakspan for cardiovascular endurance, reproductive capacity, or fluid intelligence might have ended in their late 30s.
Consequently, modern humans spend the vast majority of their adult lives in a state of continuous decline. We carry a massive, widening functional gap well before any clinical disease is ever diagnosed.
Extending Peakspan is the true functional manifestation of rejuvenative biomedical progress. It is not enough to simply delay the onset of multimorbidity. Our goal must be to stretch the “peak” phase of the human life cycle, pushing the 90% performance threshold out into our 40s, 50s, 60s, and beyond. We want to ensure that humans do not just survive, but that they operate with the vigor, resilience, and capability of their youth for as long as possible.
The Asynchronous Architecture of Human Aging
To effectively target Peakspan, we must precisely quantify the biological realities of individual organ systems. Because the human body is highly asynchronous, our therapeutic interventions cannot be uniform; they must be timed to system-specific inflections.
Cognitive Peakspan: The human brain ages in a highly segmented manner. Fluid intelligence—which dictates processing speed, fluid reasoning, and visual-spatial reasoning—hits its absolute peak rapidly, optimizing between the ages of 20 and 24, with working memory capping out at 25 to 29. This translates to a fluid cognitive Peakspan that barely survives our 20s. Conversely, crystallized intelligence, which governs verbal comprehension and vocabulary, grows and stabilizes until peaking between 45 and 54, remaining resilient against decline until age 80.
Cardiorespiratory Peakspan: Cardiovascular and respiratory capacities are equally unforgiving. Maximal aerobic capacity (VO₂max), cardiac output, and maximum heart rate reach their zenith in our early 20s. Following this brief window, VO₂max systematically declines at roughly 10% per decade. Gas-exchange efficiency, measured by DLCO, accelerates its decline past the age of 40.
Reproductive Peakspan: Nature is decidedly sexist in its application of reproductive aging. For women, the reproductive Peakspan is heavily concentrated in the 20s and early 30s. At age 30, women retain an estimated 12% of their pre-birth non-growing follicles, a number that plummets to just 3% by age 40. Men experience a more gradual decline, though peak semen quality parameters universally decline after age 40. The female reproductive system is one of the few physiological architectures that biologically drops to 0% functionality over time.
Immune Peakspan: Thymic involution, which occurs shortly after puberty, utterly collapses the output of naive T-cells. By age 25, thymic export drops to 20% of its prepubescent level, and by age 55, it operates at a mere 5%. The B-cell Peakspan is similarly truncated, operating optimally only from late adolescence to early adulthood before molecular capacities progressively halve by midlife.
Musculoskeletal, Renal, and Digestive Peakspans: Muscle strength generally peaks between 20 and 35, entering a significant decline by age 65. Renal systems show early decay, with the estimated glomerular filtration rate (eGFR) and creatinine clearance starting their decline in our early 30s. In the digestive system, hepatic unbound clearance falls by roughly 0.8% every single year starting at age 40.
When you view the aggregate data, the overarching picture is undeniable: humans naturally maintain a functional state at or above 90% capacity for a remarkably small fraction of their total lifespan.
The Macroeconomic Imperative of Peakspan
Why is extending Peakspan so critical beyond just individual human desire? Because it is strictly necessary for the survival and sustained economic growth of aging societies.
Healthcare economics often relies on a metric called QALY (Quality-Adjusted Life Year). A QALY serves as a universal score because it measures both how long you live and how well you live, representing a year lived in an optimal, healthy state. If we only focus on extending healthspan, we might add a few QALYs at the end of life by preventing a hospital stay. But if we extend Peakspan—if we keep a person operating at 90% of their peak cognitive and physical capacity for an extra 10 or 20 years—we unlock an unprecedented reservoir of human capital.
Consider this: an average surgeon performing 400 surgeries a year for 30 years generates approximately 24,000 QALYs. If we discover an entirely new drug that combats aging and adds exactly 10 years of peak, productive life to everyone on the planet, we instantly generate 80 Billion QALYs.
The Baumol effect and the massive drag of healthcare costs on developed nations are directly tied to the period of “decline.” In economics, the Baumol effect describes the tendency for wages in jobs that experience little to no productivity growth (such as nursing and manual medical care) to rise continuously, driving up the costs of these services exponentially. If people maintain their Peakspan, they remain highly productive, innovative, and economically active. They consume less reactive healthcare and contribute more to the global output, effectively neutralizing the Baumol effect on medical expenditures.

Sustained economic growth in an aging society depends critically on Rejuvenative progress (RBMTR) outpacing Non-rejuvenative progress (NBMTR). Advances that strictly extend lifespan without restoring youthful function (NBMTR) simply expand the duration of dependency. By targeting Peakspan, we prioritize Rejuvenative progress, increasing the productive capacity of the population, delaying the Biological Retirement Age, and averting the macroeconomic collapse threatened by the silver tsunami.
The “Biomedical Progress Rate” of a nation should not be measured by how many nursing homes it builds, but by how long its citizens remain at the peak of their functional performance.
Deep Aging Clocks, Life Foundation Models and Pharmaceutical Superintelligence
How do we actually achieve and measure Peakspan extension? The answer lies in generative artificial intelligence and the deployment of “Deep Aging Clocks”.
Traditionally, aging clocks assigned a biological age based on a population mean. Moving forward, AI systems must be calibrated to measure a “delta-peak age”—an alignment marker that computes functional readouts against the individual’s true personal peak rather than chronological age.
To do this, we are utilizing multimodal life models, such as the PreciousGPT framework, which learn joint embeddings across methylomes, proteomes, metabolomes, and clinical laboratories. These massive transformer networks can estimate the precise time an individual spends near their biological maxima and accurately forecast the exact timing of slope transitions—the moment they exit their Peakspan.
This capability forms the foundation of Pharmaceutical Superintelligence. We are now compressing the three-to-four-year marathon of finding a viable preclinical candidate into a 12-to-18-month sprint. For example, using our AI platform at Insilico Medicine, we designed rentosertib—a drug featuring a novel biological target and a novel molecular structure—entirely via generative AI, yielding positive clinical efficacy signals for idiopathic pulmonary fibrosis.
We are systematically shifting drug discovery from a bespoke, artisan craft into a highly scalable, compute-driven engine. We can now navigate incalculably large chemical spaces to design targeted interventions meant to maintain biological systems within that critical 90% threshold.
Architecting the Future: AI-Integrated Biotechnology Hubs
The scale of this vision requires an upgrade not just to our algorithms, but to our physical infrastructure. The traditional, fragmented approach to drug development is insufficient. We must transition to AI-Integrated Biotechnology Hubs.
These hubs are purpose-built, self-contained research ecosystems that physically unite advanced residential real estate, commercial amenities, biotechnology research facilities, and research hospitals under a centralized, AI-driven operating system. By embedding IoT biosensors directly into smart homes, we enable continuous, non-invasive health monitoring.
This creates a Multi-Sided Platform governed by Federated Learning, where AI models are trained on decentralized data sources without raw patient data ever leaving its secure environment. Through dynamic consent interfaces and data trusts, residents granularly manage their data permissions in real-time, allowing scientists to ethically aggregate high-dimensional, longitudinal data. This infrastructure transforms real estate into an active enabler of scientific progress, maximizing data utility to accelerate the discovery of interventions capable of extending Peakspan.

Extending Peakspan, Restoring Lost Function and Even Augmenting Human Performance Should Be the Ultimate Goal of Geroscience and Longevity Medicine
The transition from Lifespan to Healthspan was a monumental victory for our field. It brought us respectability, funding, and a unified voice. To all my colleagues, researchers, and physicians who champion healthspan: your work is the bedrock of everything we do.
But we are scientists, and our mandate is to push the boundaries of what is possible. With the advent of generative AI, quantum computing, and advanced geroscience, we have the tools to look beyond the mere absence of disease.
Let us embrace Peakspan. Let us systematically try to beat the biological clock for every single organ and capability. Let us measure the subtle erosions of our youth and deploy advanced, AI-discovered therapeutics to restore them.
Longevity is the ultimate form of prosperity and freedom. It is time we start fighting not just for the right to live without disease, but for the right to live at our absolute peak.
Longevity is the new form of prosperity, my friends. Live long, peak long and prosper!
We need to, and already are aiming beyond our youthful peak. "Peakspan" still falls short of defining the increasingly transhumanist future, and does not even clearly supercede healthspan as it is popularly - if imprecisely - understood. Why bother with a new word that adds so little? Maybe you could redefine it in your next paper to be something greater than partial restoration of best-to-date? ...Or maybe just get back to creating the means by which we will achieve superhumanity.
How about designing ways to stop the loss of the peak span? The human body is a perfect system designed to function at peak span for ever. It is the way of life that our societies induce that provoques de functional decay. Humans get lost in ambitious ideals of power and forget the power within.