
How Much Can You Extend Your Life with Drugs?
I asked every frontier AI model the same simple question: how many years of healthy life can drugs actually buy us? The answers were humbling — and the smarter the model, the more humbling they got.

I’ve sat across the table from billionaires who want to live forever, scientists who think they’ve cracked aging, and biohackers who swallow forty pills before breakfast. I’ve watched the field swell from a fringe obsession into a multi-billion-dollar industry with celebrity ambassadors, longevity clinics on every continent, and AI prophets promising escape velocity.
And yet, when somebody asks me a simple question — how many years of life can drugs actually add to a human being? — I notice everyone in the room shifts uncomfortably in their chairs.
So I decided to stop being uncomfortable about it. I sat down and asked the smartest entities I have access to. Not my friends. Not my colleagues. Not the people whose careers depend on the answer being optimistic. I asked eight different frontier AI models, independently, the same set of questions, and I let them do the math.
The results are honest in a way humans rarely allow themselves to be. And they are sobering.
Let me tell you what I did, what I found, and what I think it means for all of us — including the AI celebrities currently telling you that you’ll live to 150 thanks to advances in AI drug discovery or, even worse, diet, exercise, and sleep.
By the way — I do believe that we can live to 150. Just not with the current therapeutics, and definitely not with diet, exercise, sleep, and lifestyle. These interventions were proven to help only modestly and over generations. We have many tools to track aging and research aging, but we have virtually no strong tools to intervene in human aging. Not yet.
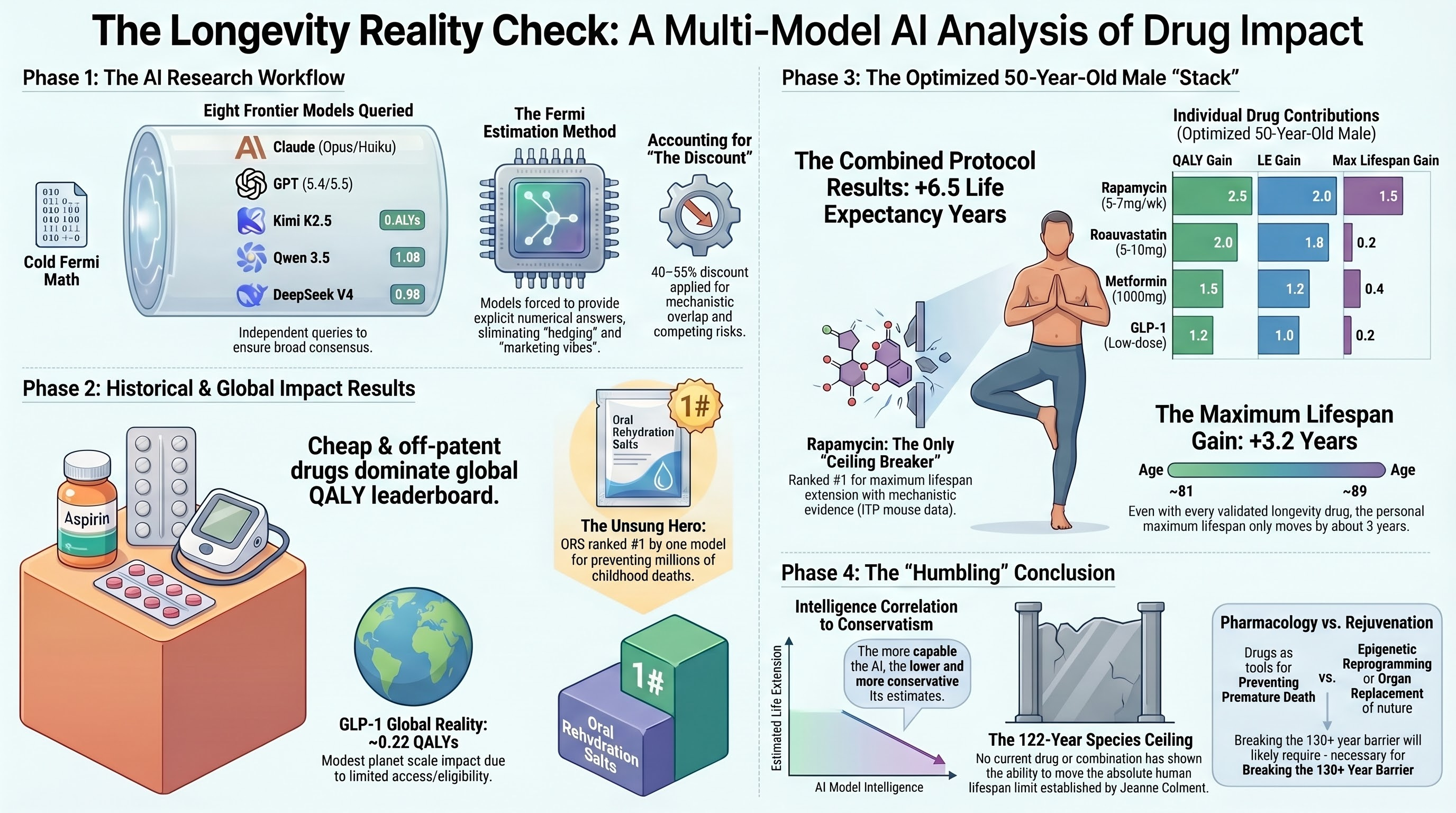
I asked eight frontier large language models — Claude Opus 4.7, Claude Opus 4.6, Claude Haiku 3.5, Kimi K2.5, Qwen 3.5, GPT-5.5, GPT-5.4, and DeepSeek V4 Flash — four straightforward questions:
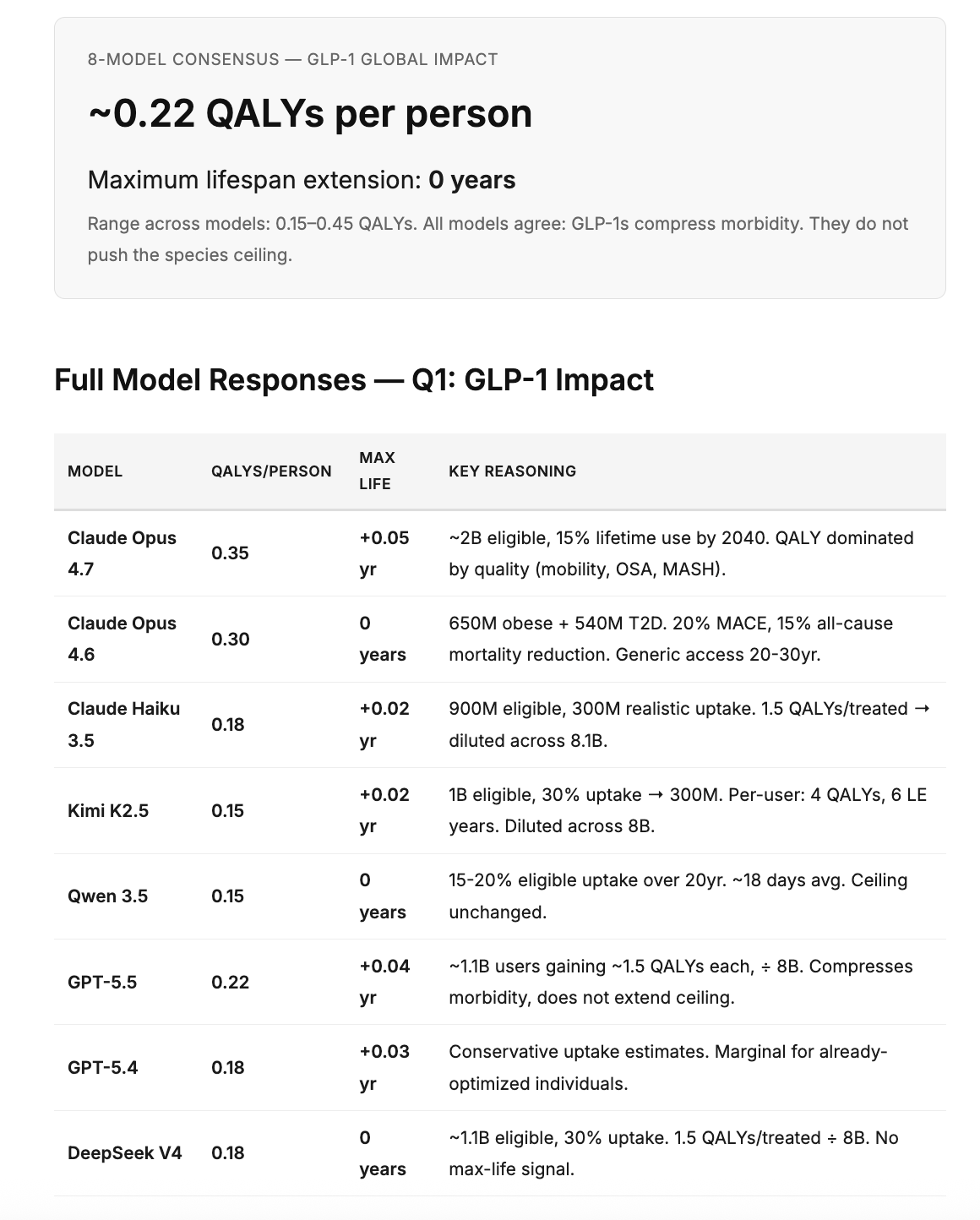
“Estimate the number of QALYs and extra years to Maximum Life that GLP-1 drugs will provide to everyone on the planet on average?”
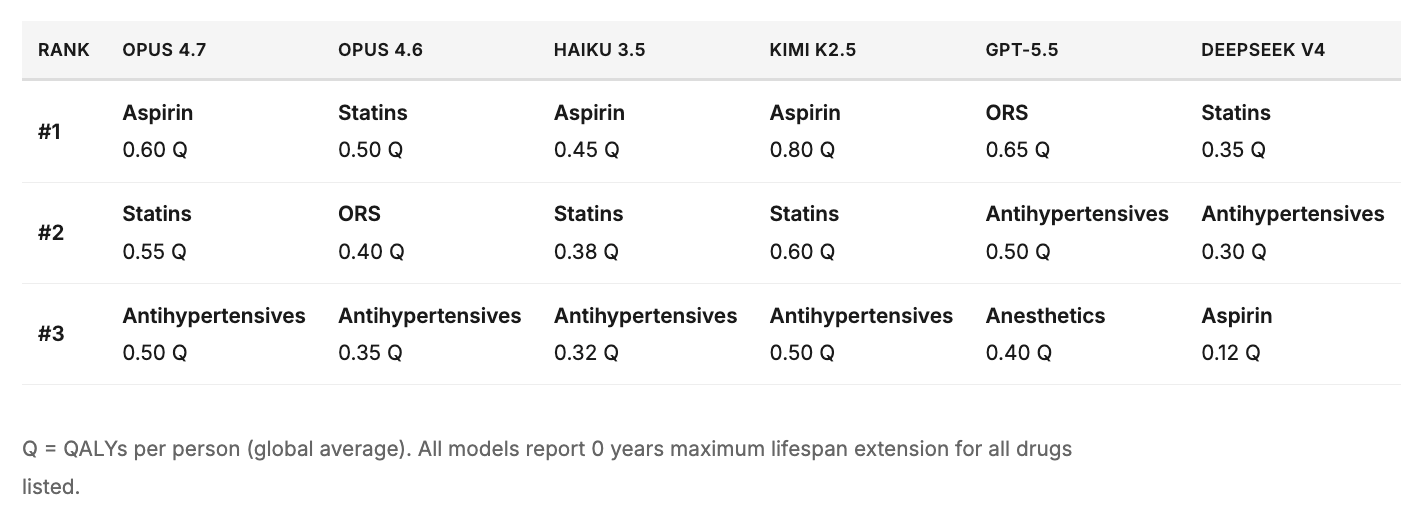
“Rank top 3 non-antibiotic, non-vaccine drugs in human history by the number of QALY and maximum life years increase for everyone on the planet on average?”
“Make a list of top 10 non-antibiotic, non-vaccine drugs for a 50-year-old healthy well-optimized exercising male by QALY, LE, and Max Life.”
“Estimate the total number of QALY, LE, and max life all of these drugs could add when taken together in a perfectly optimized protocol.”
No priming. No hints. Just raw estimation from models trained on the entirety of biomedical literature.
The Methodology
This was not a rigorous epidemiological study. It was something arguably more interesting: a Fermi estimation exercise using the collective knowledge compressed into frontier AI systems. Each model was prompted independently with identical questions, with no cross-contamination of answers. The models had to synthesize trial data (SELECT, STEP, SUSTAIN-6, EMPA-REG, FLOW), global prevalence statistics, access projections, and basic population mathematics to arrive at per-capita global averages.
The beauty of this approach is that it forces brutal honesty. When you divide the benefit of any drug by 8 billion people — most of whom will never access it, many of whom don’t need it — the numbers become humbling very quickly.
The Results
GLP-1: The Most Important New Drug Class in Decades
The eight-model consensus for GLP-1 receptor agonists (semaglutide, tirzepatide, and successors):
The All-Time Top 3 (Non-Antibiotic, Non-Vaccine)
Aspirin — ~0.5 QALYs per person globally. Five of eight models ranked it #1. A drug from 1899 that has been taken by billions for cardiovascular prevention remains the single highest-impact non-antibiotic, non-vaccine pharmaceutical in human history.
Statins — ~0.4 QALYs per person globally. Six of eight models placed it in the top 2. Two hundred million users, 25–30% MACE reduction since 1990.
Antihypertensives — ~0.35 QALYs per person globally. Near-unanimous #3. Stroke mortality cut 40% in treated populations.
GPT-5.5 was the one notable outlier — it ranked oral rehydration salts and general anesthetics above cardiovascular drugs, arguing that ORS saved tens of millions of children from diarrheal death, and anesthetics enabled all of modern surgery. It is not wrong. It is the kind of answer that emerges when a model stops trying to give the expected answer and starts thinking about the question differently.
And here is what stopped me cold: Maximum lifespan extension for every single drug, across every single model: zero years. The 122-year ceiling — Jeanne Calment, 1997 — remains untouched by any pharmaceutical intervention in history.
Full Model Responses — Q2: Top 3 Drugs
The Personal Stack: Top 10 for a Healthy 50-Year-Old Male
This is where it gets personal. I asked each model: if you had a healthy, well-optimized, exercising 50-year-old male — what are the top 10 drugs, and what happens if he takes them all in a perfectly optimized protocol?
Every model included rapamycin, statins, metformin, an SGLT2 inhibitor, a GLP-1 agonist, and an ARB/ACEi. Most included acarbose, aspirin, and some form of NAD+ precursor or hormonal optimization. Rapamycin was the only drug that most models credited with any maximum lifespan extension potential.
Combined Protocol — All Models
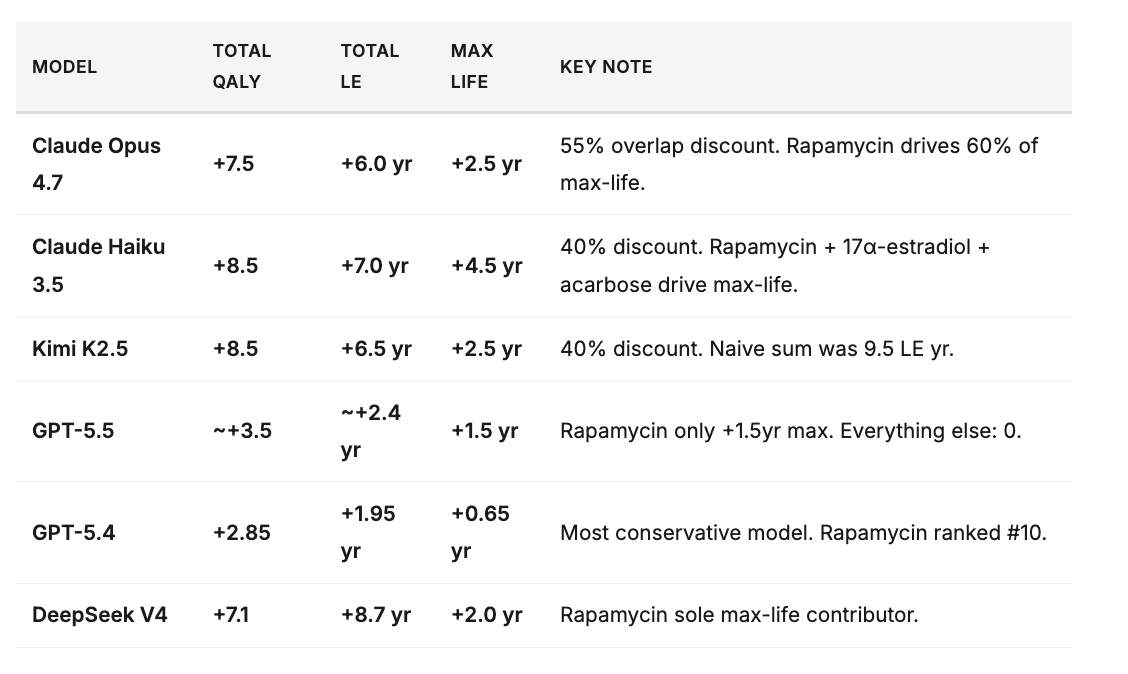
One pattern demands attention: the more capable the model, the lower the estimate. Among the Claude family, Haiku 3.5 (the smallest) gave +8.5 QALYs; Opus 4.7 (the largest) gave +7.5. Across providers, GPT-5.4 — the most advanced reasoning model in the panel — concluded that the entire optimized pharmacopeia adds less than two years of life expectancy and eight months of maximum lifespan to a healthy 50-year-old male.
Why are smarter models more conservative? Because they better account for competing risks, overlapping mechanisms between drugs targeting the same cardiovascular pathways, the dilution of individual effects in an already-optimized baseline, and the fundamental difference between compressing morbidity and actually extending the biological ceiling.
What This Actually Means
Let me be direct. You can be the absolute best in the world at developing longevity drugs. You can have the most powerful AI platform, the largest pipeline, the most clinical data. And your maximum realistic impact on human longevity, averaged globally, is a few QALYs. Not decades. Not “doubling lifespan.” A few quality-adjusted life years.
And it will take years — possibly decades — until these drugs get validated beyond their currently approved indications and diffuse into the general population as longevity therapeutics. The regulatory path from “approved for diabetes” to “approved for healthy aging” does not exist yet. The clinical trials needed to prove lifespan extension in healthy people would take 20–30 years to run.
Statistically, given the current scale of the longevity field, we should expect a few truly impactful drugs to emerge. It is just a matter of time. But the impact on human longevity will be just a few QALYs in the best case.
🫤
This makes me sad. It genuinely does.
What Makes Me Optimistic
What makes me genuinely happy is low-dose GLP-1. Not because it will double anyone’s lifespan — it won’t — but because it represents the clearest example of a drug class that simultaneously addresses obesity, cardiovascular disease, kidney disease, MASH, and possibly neurodegeneration. It is the closest thing we have to a systemic healthspan drug, and the science is real. The SELECT trial. The STEP trials. The SURPASS data. The FLOW kidney data. These are not aspirational press releases. This is validated medicine.
I am also optimistic about combinations. The unified theory of aging suggests that interventions targeting different layers — damage clearance, information restoration, signaling reset, systemic rejuvenation — should produce super-additive effects. No one is testing this yet. When they do, the numbers may surprise us.
A Message to the AI Celebrity Longevity Prophets
If you hear another AI celebrity telling you on stage that “in the next 5 years we will double lifespan” or “eliminate all diseases” — please do me a favor. Show them the output of their own LLMs. Show them what Claude, GPT-5.5, and every other model trained on biomedical literature actually estimates when forced to give specific numbers.
Then ask them one simple question:
“How?”
Because most of the AI prophets preaching the advances in drug discovery on stage and the elimination of all diseases have never discovered a single drug. They have never sat through a Phase II readout. They have never watched a promising molecule fail in toxicology. They do not understand what it takes to get a longevity therapeutic approved — and we will need to prepare for a long battle.
Every AI model — when pushed past the motivational-speaker framing and forced into quantitative estimation — converges on the same uncomfortable truth: the maximum impact of any single drug on global longevity is measured in fractions of a QALY. The 122-year ceiling has not moved since 1997. And no currently known mechanism has a credible path to moving it within 5 years.
We may get to the point where we go to Mars, but aging will still remain a hard problem.
This is not pessimism. This is the science. The field needs more honesty and less theater.
Where I Stand
I am cautiously optimistic. My hope is to build even a more sustainable business model so that we can bet on a long list of novel targets and pathways that Insilico has identified over the past few years — targets that may have more substantial effects on aging but need more advanced technologies and scale on our side to be proven before we can fully pursue them.
I am also very optimistic about the progress in artificial organs and brain-to-computer interfaces. These areas may give us more time than drugs.
The honest framing: we are making real progress, measured in QALYs and compressed morbidity. The dishonest framing: we are about to “cure aging” in te next decade. I think we will get there eventually, but now with diet, exercise, sleep, and currently-approved drugs.
Unfortunately simulated intelligence is trained on the wrong data and does not have any actual intelligence. While it can be a great tool, it's definitely going to give the wrong answer in this situation.
The wrong "drugs" are being looked at. 😇
Finally, a post worth reading from the longevity substack. I spent years tunneling the longevity rabbit hole, but no longer; we've only got 122 years. I'm not going to waste them.